The Omega-3, Omega-6 Fatty Acid Controversy; Do They Work?
- FibonacciMD

- Dec 22, 2022
- 13 min read
Updated: May 10, 2023
Nutrition and Integrative Medicine summary article on Omega Fatty Acids.
Nutrition and Integrative Medicine

InReview
Contributors- Rich Strongwater, MD and
According to the 2012 National Health Interview and Nutrition Examination Survey, fish oil is one of the most commonly used nonvitamin/nonmineral dietary supplements in the United States. In 2012, 7.8 % of adults reported using fish oil supplements.[1] There are multiple reasons for people taking fish oil supplementation which include improving heart health and reducing symptoms of rheumatoid arthritis. However, definitive evidence supporting its use is lacking for some of the indications it is taken for. This article will discuss the effectiveness or lack of efficacy of both adequate omega fatty acid dietary intake as well as prescription omega fatty acid supplements.
Omega Fatty acids
The human body does not produce any omega-3 or omega-6 fatty acids which are considered essential polyunsaturated fats and must be obtained from dietary sources.
There are three types of omega-3 fatty acids (also called n-3 fatty acids): eicosapentaenoic acid (EPA), docosahexaenoic acid (DHA), and alpha-linolenic acid (ALA). EPA and DHA are found in fatty fish such as wild salmon, lake trout, sardines, anchovies, striped bass, and Arctic char. ALA is the plant form of omega-3 fatty acids found in foods such as flax meal, chia seeds, walnuts, and flax seed oil. There is only limited conversion of ALA to EPA or DHA in the body.
The omega fatty acids are an important part of cell membranes and affect the function of the cell receptors in these membranes. They provide the starting point for making hormones that regulate blood clotting, contraction and relaxation of artery walls, and reduce inflammation. They also bind to receptors in cells that regulate gene expression.[2,3] DHA is one of the key nutrients in the development and the maturity of the brain and eyes in utero and infancy.[4]
Sources of omega-6 include vegetable oils used in cooking such as corn, safflower, sunflower, or soybean oils, as well as hydrogenated oils found in margarine and vegetable shortening, and meat from livestock animals and poultry raised on grain rather than pasture greens.[5] While some omega-6 is needed for health and normal cell membranes, it is felt that too much omega-6 can lead to a pro-inflammatory condition which may actually worsen health.[5]
Omega-6 fatty acids include linoleic (LA) and arachnologic acid. LA helps with structural integrity of the skin and is a part of the lipid skin barrier. LA intake, when substituted for saturated fatty acids, reduces blood cholesterol and low-density lipoprotein (LDL)-cholesterol concentrations partially due to its inhibition of proprotein convertase subtilisin kexin type 9 (PCSK9).[6] A systematic review and meta-analysis found that the replacement of 5% of saturated fatty acids by LA was associated with a 9% reduction in coronary heart disease.[6,7] In another meta-analysis, higher levels of LA were associated with a lower risk of major cardiovascular events [6,8].
Omega-6 to Omega-3 Ratio
The ratio of omega-6 to omega-3 fats in our ancestor’s diet was about 1:1 and presently in industrialized countries with the rise of the use of vegetable oils high in omega-6, the ratio of omega-6 to omega-3 is typically around 15:1 or higher, which is thought to be proinflammatory with negative effects on health.[9,10] It has been suggested that a 4:1 ratio of omega-6 to omega-3 intake may be optimal. The actual optimal ratio to target may differ depending on what condition is being treated, but there is evidence that lowering the omega-6 to omega-3 ratio can reduce cardiac mortality, decrease rectal cell proliferation in colorectal cancer patients, and lessen inflammation in patients with rheumatoid arthritis.[10]
Health Benefits
A multitude of possible health benefits of omega-3 fatty acids have been found in research studies. The most impressive benefits have been the findings for reducing triglyceride levels and preventing heart disease. Many disease entities have been studied to see if omega-3 fatty acid treatment will help. These include cancer prevention, Alzheimer’s disease and dementia, macular degeneration, dry eye disease, rheumatoid arthritis, infant health and development, depression, inflammatory bowel disease, childhood allergies, attention-deficit/hyperactivity disorder, and cystic fibrosis.[11,12]
Heart disease
There are some Cochrane Database meta-analyses on the use of fatty acids for heart disease. In 2018 one review concluded that increased use of polyunsaturated fatty acids such as omega-3 and omega-6 “probably slightly reduces risk of coronary heart disease and cardiovascular disease events, may slightly reduce risk of coronary heart disease mortality and stroke, but has little or no effect on all‐cause or cardiovascular disease mortality. The mechanism may be via triglyceride reduction.”[13] Another Cochrane review on the use of omega-3 fats concluded that while having no effect on overall mortality, increasing EPA and DHA intake slightly reduced the risk of coronary artery heart disease events and mortality, and reduces serum triglycerides. They also reported that increasing ALA may slightly reduce the risk of cardiovascular events and arrhythmias. The authors calculated the number needed to treat, based on the data, and found that 167 people would need to increase their EPA and DHA intake to prevent one coronary event and 334 people would need to increase their EPA and DHA intake to prevent one death from coronary disease. 500 people would need to increase their ALA intake to prevent one coronary event and 91 people would need to increase their ALA intake to prevent one person from having an arrhythmia.[14]
Academic Performance in Children
Research has also been conducted with omega-3 fatty acids and childhood- academic performance. In a trial in the European Journal of Clinical Nutrition, 239 children were randomized to receive tuna fish oil (high in omega-3 fatty acids or sunola oil (low in omega-3 fatty acids ) daily from age six months to five years. The authors concluded that their findings did not support administering fatty acids to children to improve academic performance.[15]
NIH Conclusions
The National Institutes of Health (NIH) has researched some of the uses of omega-3 supplementation as treatment, which are copied or summarized below.[11]
Infant Health and Neurodevelopment
Observational studies of maternal DHA consumption during pregnancy and breastfeeding found that eating 8 ounces per week of seafood that contains DHA is associated with better infant health outcomes. The 2015–2020 Dietary Guidelines for Americans states that women who are pregnant or breastfeeding should consume 8–12 ounces of seafood per week, choosing from varieties that are higher in EPA and DHA and lower in methyl mercury, such as salmon, herring, sardines, and trout. They should not consume king mackerel, shark, swordfish, and tilefish that are high in methyl mercury, and limit the amount of tuna they consume to 6 ounces a week. Most infant formulas in the U.S. contain DHA and arachidonic acid, however, there is currently insufficient definitive evidence supporting the positive benefits of use in infant formulas.
Cancer
Breast Cancer- Evidence from several observational studies suggests that higher intakes of omega-3s are associated with a lower risk of breast cancer, but more clinical trials are needed to confirm this finding.
Colorectal cancer: Limited evidence from observational studies suggests that greater consumption of fish and omega-3s is associated with a reduced risk of colorectal cancer.
Prostate cancer: Several prospective and case-control studies have investigated associations between either blood levels or intakes of omega-3s and risk of low-grade or high-grade prostate cancer. Results from these studies have been inconsistent, with some showing benefit and others no benefit.
With respect to cancers in general, the NIH concludes that data from observational studies show no consistent relationship between omega-3s and overall cancer risk, but more studies are needed. Although some evidence suggests that higher omega-3 intake reduces the risk of breast and possibly colorectal cancers, a large clinical trial found that omega-3 supplements did not reduce the overall risk of cancer or the risk of breast, prostate, or colorectal cancers.[16]
Cognitive function
Omega-3 supplementation does not affect cognitive function in healthy older adults or in people with Alzheimer’s disease compared to placebo. For people with mild cognitive impairment, it may improve certain aspects of cognitive function, including attention, processing speed, and immediate recall.
Age-related Macular Degeneration (AMD)
Although there is some evidence dietary DHA decreased the incidence of AMD, a Cochrane review concluded that omega-3 supplementation in people with AMD does not reduce the risk of progression to advanced AMD or moderate to severe vision loss.[17]
Dry Eye Disease
Evidence to date shows no consistent relationship between omega-3s and dry eye disease.
Rheumatoid Arthritis
Findings suggest that omega-3s may be helpful as an adjunctive treatment to pharmacotherapy for ameliorating the symptoms of rheumatoid arthritis. However, more research is needed to confirm this finding.
Depression
A Cochrane review found insufficient evidence to determine whether omega-3s are beneficial for major depressive disorders. The authors did find a small-to-modest beneficial effect on depressive symptoms but concluded that the effect was not clinically significant.[18]
Inflammatory Bowel Disease
Available evidence does not support the use of omega-3 supplements to treat active or inactive inflammatory bowel disease.
Childhood allergies (Including Asthma)
A Cochrane review concluded that there is limited evidence to support the use of omega-3 supplements by women during pregnancy and/or lactation for reducing the risk of allergic disease in their children. Another meta-analysis concluded that the results were suggestive of a protective association between higher maternal intakes of omega-3s or fish and incidence of allergic disease symptoms in the offspring.[19]
Cystic fibrosis
A Cochrane review found that omega-3s might improve lung function and increase blood levels of essential fatty acids in people with cystic fibrosis, but there is not enough evidence to recommend routine use to treat cystic fibrosis patients.[20]
Premature Labor
One meta-analysis concluded that DHA supplementation did not decrease premature births, but resulted in a slight increase gestational latency (Time from rupture of membranes until delivery.) and birth weight.[21]
Omega-3 Prescription Supplements
In 2019, the FDA announced it would allow certain qualified health claims on products stating that consuming EPA and DHA omega-3 fatty acids in food or dietary supplements may reduce the risk of hypertension and coronary heart disease. However, the FDA stated that the evidence is inconsistent and inconclusive.[22]
Omega 3 fatty acids (OM3FA) prescription brands made from fish oils[23]
Icosapent ethyl and omega-3-acid ethyl esters are approved for adults with very high triglyceride levels (≥ 500 mg/dl) as an adjunct to diet to decrease triglyceride levels and reduce cardiovascular events.
Lovaza or Omtryg (omega-3-acid ethyl esters). These contain a combination of ethyl esters of omega-3 fatty acids, principally EPA and DHA. Typical daily dose is 4 grams/day either as 4 capsules once a day with meals or two capsules twice a day with meals.
Vascepa (icosapent ethyl) contains only EPA. The typical daily dose is 4 grams/day taken as two, 2-gram capsules twice a day with meals
All OM3FA supplements should be taken whole without being crushed, chewed, or dissolved in the mouth.
Adverse Effects[23]
The FDA-approved fatty acid prescriptions are generally safe with benign side effects such as fishy taste, eructation, dyspepsia, diarrhea, gas, nausea, and arthralgia.
There is a warning in the prescribing information of the omega-3-acid ethyl esters Lovaza and Omtryg of a possible association with more frequent recurrences of symptomatic atrial fibrillation or flutter in patients with paroxysmal or persistent atrial fibrillation, particularly within the first months of initiating therapy.[24,25]
Contraindications[23]
While omega-3 fatty acid supplements are not considered allergenic, the FDA recommends caution in patients allergic to seafood.
Monitoring[23]
Omega-3 fatty acids may reduce platelet activity and periodic monitoring is recommended for patients on anticoagulants or anti-platelet medications.
It is recommended that the LDL cholesterol be monitored for patients taking the DHA-containing products omega-3-acid ethyl esters, due to DHA’s association with an increase in LDL cholesterol.[8] In patients with dyslipidemia, icosapent ethyl may be a better option as it has no association with increased LDL cholesterol.
For patients with hepatic impairment, monitoring of the AST and ALT should be performed.
In patients with paroxysmal or persistent atrial fibrillation, the prescription products containing omega-3-acid ethyl esters have a possible association with increased recurrences of symptomatic atrial fibrillation or flutter.
Physicians should inquire about patients' diets to ensure proper DHA and EPA levels are achieved and fish high in methyl mercury are avoided.
Toxicity[23]
The FDA-approved omega-3 fatty acid prescriptions are pregnancy category C drugs, and it is unknown if the drug can cause fetal harm or can affect reproductive capacity.
Methylmercury, which can be toxic, is found in some fish. Individuals who use fish as their primary source of omega-3 or pregnant and nursing women should limit their intake to two to four servings of fish a week and replace fish that are high in methyl mercury, such as swordfish, albacore tuna, dolphinfish, kingfish, and shark with fish that contain a lower amount of methylmercury, such as salmon, herring, sardines, and trout. DHA and EPA prescription supplements do not contain methylmercury.
Dietary Intake Versus Prescription Supplementation of Omega Fatty Acids.
It is generally recommended to get omega-3 and omega-6 from dietary sources. Supplementation in the form of medication may be beneficial for certain groups in treating specific disease entities, such as cardiac patients or those with elevated triglycerides.
Supplementation may also be considered if dietary intake is inadequate, such as in pregnant or breast-feeding vegans or vegetarians, after consultation with a health care provider and a review of omega-3 dietary intake.[26] It is recommended that nursing mothers require 200 to 300 mg DHA intake per day from dietary sources with consumption of 1 to 2 portions of fish per week (such as herring, canned light tuna, or salmon) to guarantee a sufficient concentration of DHA in the breast milk and may only need to take DHA supplements if they are malnourished or on a vegan diet.[27]
Adequate Intake Levels
There are no recommended dietary allowances for omega-3 and omega-6 due to insufficient data. There are adequate intake (AI) levels set by the Food and Nutrition Board of the Institute of Medicine (IOM) (now called the National Academy of Medicine). There are no specific recommendations for DHA or EPA by the IOM, [11,27]
Omega-3 AI levels (ALA in adults, total omega-3s under one year of age)
Age | Male | Female | Pregnancy | Lactation |
Birth to 6 months* | 0.5 g | 0.5 g | | |
7–12 months* | 0.5 g | 0.5 g | | |
1–3 years** | 0.7 g | 0.7 g | | |
4–8 years** | 0.9 g | 0.9 g | | |
9–13 years** | 1.2 g | 1.0 g | | |
14–18 years** | 1.6 g | 1.1 g | 1.4 g | 1.3 g |
19-50 years** | 1.6 g | 1.1 g | 1.4 g | 1.3 g |
51+ years** | 1.6 g | 1.1 g | | |
*As total omega-3s **As ALA(over 1year of age) [10]
Omega-6 AI levels[28]
For Infants | 0-6 months | Omega-6 FA* | Male 4.4 g | Female 4.4 g |
Infants | 7-12 months | Omega-6 FA* | 4.6 g | 4.6 g |
Children | 1-3 years | LA** | 7 g | 7 g |
Children | 4-8 years | LA | 10 g | 10 g |
Children | 9-13 years | LA | 12 g | 10 g |
Adolescents | 14-18 years | LA | 16 g | 11 g |
Adults | 19-50 years | LA | 17 g | 12 g |
Adults | 51 years and older | LA | 14 g | 11 g |
Pregnancy | all ages | LA | ----- | 13 g |
Breast-feeding | all ages | LA | ----- | 13 g |
*Omega-6 fatty acids present in human milk can contribute to the AI for infants. ** LA = linoleic acid
Dietary Sources of Omega-3 and Omega-6
Sources of omega-3 include:
● Fish and other seafood (salmon, mackerel, tuna, seabass, herring, sardines)
● Soybeans and edamame
● Kidney beans
● Nuts and seeds (flaxseed, chia seeds, hemp seeds, walnuts)
● Seaweed and algae
● Wheat germ
● Fortified foods (eggs, yogurt, juices, milk, soy beverages)
Omega-3 Levels in Selected Foods
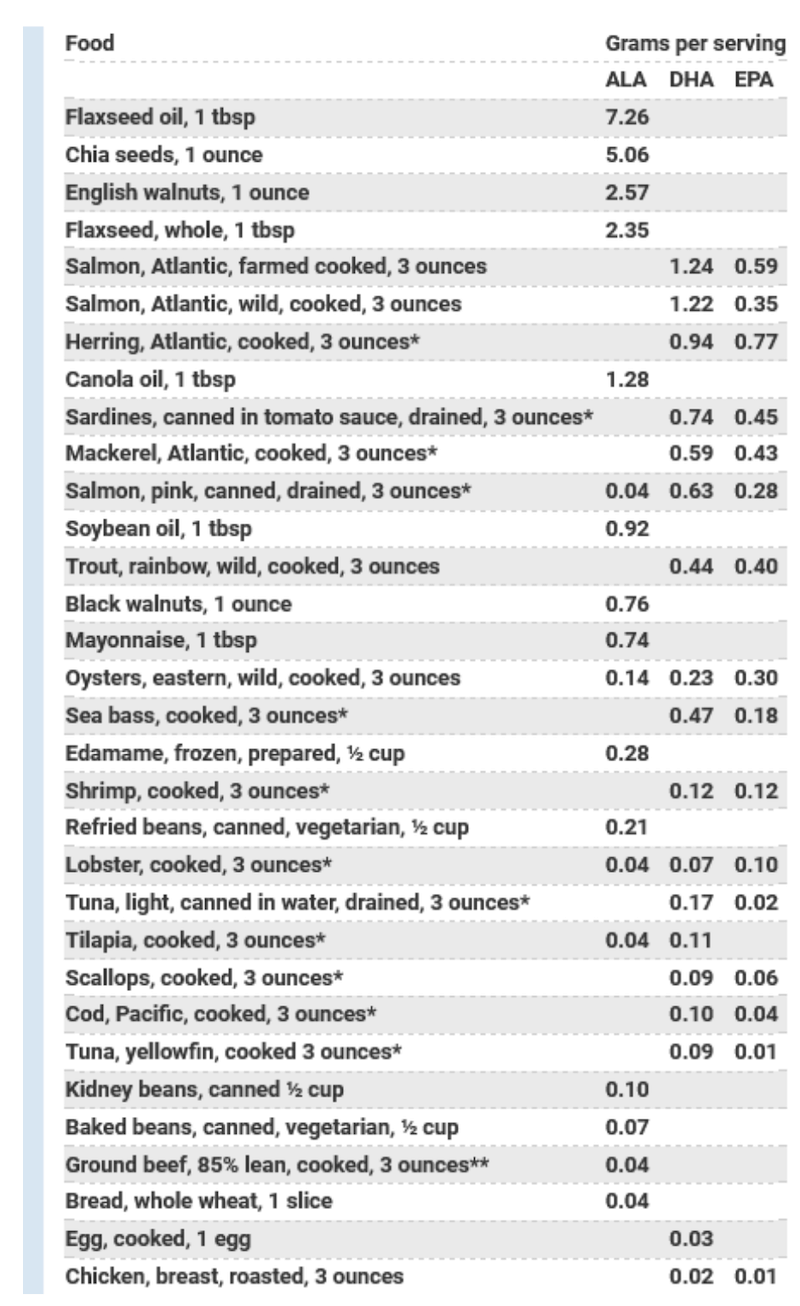
[11]
Sources of omega-6 include:
● Eggs
● Meat, Poultry
● Whole grain breads
● Cereals
● Oils, such as sunflower, safflower, sesame, grapeseed, soybean, corn
● Seeds, such as: pumpkin, sunflower
● Chickpeas and legumes
● Nuts, including pignolia (pine), almonds and pistachios
Estimates of Amounts and Ratios of Omega-6 and Omega-3 in Selected Foods in gms/100gms, Unless Otherwise Indicated.
| Omega-6 | Omega-3 | Omega-6:3 ratio |
Corn oil | 49.83 | 0.6 | 83.05 |
Sunflower Oil | 49.89 | 0.33 | 151 |
Soybean Oil | 51.36 | 7.6 | 6.76 |
Canola Oil | 18.65 | 9.15 | 2.03 |
Olive Oil *see below | | | |
Salmon | 0.2 | 2.17 | 0.09 |
Trout | 0.42 | .75 | 0.56 |
Broccoli | 0.03 | 0.11 | 0.27 |
Kale (g/1 cup) | 0.02 | 0.03 | 0.67 |
Corn (g/1 cup) | 0.51 | 0.01 | 51 |
Walnuts | 34.02 | 6.64 | 5.12 |
Almonds | 10.54 | 0.3 | 35.13 |
Flax seed (g/1TBS) | 0.41 | 1.6 | 0.26 |
Chia seed | 5.84 | 17.83 | 0.32 |
Peanuts | 17.2 | .01 | 1,720 |
Chicken breast (g/4oz) | 0.93 | 0.11 | 8.45 |
Sirloin steak (g/4oz) | .23 | 0.04 | 5.75 |
Potato chips (g/1oz) | 6.53 | 0.01 | 653 |
Chickpeas (g/1 cup) | 1.53 | 0.06 | 25.5 |
Oatmeal (g/1 cup) | 0.92 | 0.04 | 23 |
2 Eggs | 1.18 | 0.07 | 16.86 |
2 Eggs, omega-3-enriched | 1.13 | 0.23 | 4.91 |
[29,30]
*Olive oil -The omega-6:3 ratio varies by olive species used. Most typically the ratio quoted is about 10:1 in multiple sources, but it depends on the olives used and how ripe the olives are when they are picked. (The omega-6:3 ratio ranged from about 3:1 to 21:1 in one study of Italian olives depending on the olive species.)[31,32,33]
Conclusion
Omega-3 and omega-6 fatty acids both appear to have some health benefits. However, when intake of omega-6 far exceeds omega-3, this may be pro-inflammatory and may reverse some of the benefits of the omega-3 anti-inflammatory effects. Pending further research some recommendations include:
Obtaining omega-3 and omega-6 from food sources rather than from supplementation as much as possible, unless being treated for a specific disease process or unable to get enough from diet alone.
Replacing saturated fats with omega-3 and omega-6 fatty oils, and limiting intake of very high omega-6 to omega-3 ratio oils such as corn oil and sunflower oil.
Trying to decrease some omega-6 intake and maintaining a more favorable ratio of omega-6 to omega-3 intake, such as the 4:1 ratio.
More information in our FibonacciCOMPENDIUM
References
[1] Clarke TC, Black LI, Stussman BJ, Barnes PM, Nahin RL. Trends in the use of complementary health approaches among adults: United States, 2002–2012. National health statistics reports; no 79. Hyattsville, MD: National Center for Health Statistics. 2015. Retrieved from: https://www.cdc.gov/nchs/data/nhsr/nhsr079.pdf
[2] Omega-3 Fatty Acids: An Essential Contribution. The Nutrition Source. Harvard T. H. Chan School of Public Health. 2022. Retrieved from: https://www.hsph.harvard.edu/nutritionsource/what-should-you-eat/fats-and-cholesterol/types-of-fat/omega-3-fats/
[3] Hussey B, Lindley MR, Mastana SS. Omega 3 fatty acids, inflammation and DNA methylation: an overview, Clinical Lipidology, 12:1, 24-32. 2017. Retrieved from: https://www.tandfonline.com/doi/full/10.1080/17584299.2017.1319454
[4] Li J, Pora BLR, Dong K, Hasjim J. Health benefits of docosahexaenoic acid and its bioavailability: A review. Food Sci Nutr. 2021;9(9):5229-5243. Published 2021 Jul 23. Retrieved from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8441440/
[5] Mariamenatu AH, Abdu EM. Overconsumption of Omega-6 Polyunsaturated Fatty Acids (PUFAs) versus Deficiency of Omega-3 PUFAs in Modern-Day Diets: The Disturbing Factor for Their "Balanced Antagonistic Metabolic Functions" in the Human Body. J Lipids. 2021;2021:8848161. Published 2021 Mar 17. Retrieved from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7990530/
[6] Djuricic I, Calder PC. Beneficial Outcomes of Omega-6 and Omega-3 Polyunsaturated Fatty Acids on Human Health: An Update for 2021. Nutrients. 2021;13(7):2421. Published 2021 Jul 15. Retrieved from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8308533/
[7] Farvid MS, Ding M, Pan A, et al. Dietary linoleic acid and risk of coronary heart disease: a systematic review and meta-analysis of prospective cohort studies. Circulation. 2014;130(18):1568-1578. Retrieved from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4334131/
[8] Marklund M, Wu JHY, Imamura F, et al. Biomarkers of Dietary Omega-6 Fatty Acids and Incident Cardiovascular Disease and Mortality. Circulation. 2019;139(21):2422-2436. Retrieved from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6582360/
[9] Simopoulos AP. Evolutionary aspects of diet, the omega-6/omega-3 ratio and genetic variation: nutritional implications for chronic diseases,
Biomedicine & Pharmacotherapy, Volume 60, Issue 9, 2006, Pages 502-507. https://www.sciencedirect.com/science/article/abs/pii/S0753332206002435?via%3Dihub
[10] Simopoulos AP. The importance of the ratio of omega-6/omega-3 essential fatty acids. Biomed Pharmacother. 2002;56(8):365-379. Retrieved from: https://pubmed.ncbi.nlm.nih.gov/12442909/
[11] Omega-3 Fatty Acids Fact Sheet for Health Professionals. NIH. Updated: July 18, 2022. Retrieved from: https://ods.od.nih.gov/factsheets/Omega3FattyAcids-HealthProfessional/
[12] Omega-3 Fatty Acids Fact Sheet for Consumers. NIH. Updated: July 18, 2022. Retrieved from: https://ods.od.nih.gov/factsheets/Omega3FattyAcids-Consumer/
[13] Abdelhamid AS et al. Polyunsaturated fatty acids for the primary and secondary prevention of cardiovascular disease. Cochrane Database Syst Rev. 2018 Nov 27;11(11):CD012345. Retrieved from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6517012/
[14] Abdelhamid AS, Brown TJ, Brainard JS, et al. Omega-3 fatty acids for the primary and secondary prevention of cardiovascular disease. Cochrane Database Syst Rev. 2020;3(3):CD003177. Retrieved from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7049091/
[15] Brew, B., Toelle, B., Webb, K. et al. Omega-3 supplementation during the first 5 years of life and later academic performance: a randomised controlled trial. Eur J Clin Nutr 69, 419–424 (2015). Retrieved from: https://www.nature.com/articles/ejcn2014155
[16] Manson JE, Cook NR, Lee IM, et al. Marine n-3 Fatty Acids and Prevention of Cardiovascular Disease and Cancer. N Engl J Med. 2019;380(1):23-32. Retrieved from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6392053/
[17] John G Lawrenson, JG, Evans JR. Omega 3 fatty acids for preventing or slowing the progression of age‐related macular degeneration. Cochrane Database of Systematic Reviews. 09 April 2015. Retrieved from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7087473/
[18]Appleton KA et al. Omega‐3 fatty acids for depression in adults. Cochrane Database of Systematic Reviews. 24 November 2021. Retrieved from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5321518/
[19] Gunaratne AW, Makrides M. Collins CT. Maternal prenatal and/or postnatal n‐3 long chain polyunsaturated fatty acids (LCPUFA) supplementation for preventing allergies in early childhood. Cochrane Database of Systematic Reviews. 22 July 2015. Retrieved from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8783748/
[20] Watson H, Stackhouse C. Omega‐3 fatty acid supplementation for cystic fibrosis. Cochrane Database of Systematic Reviews. 10 April 2020. Retrieved from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7147930/
[21] Saccone G, Berghella V. Omega-3 supplementation to prevent recurrent preterm birth: a systematic review and metaanalysis of randomized controlled trials. American Journal of Obstetrics and Gynecology. Volume 213, Issue 2,
2015, Pages 135-140. Retrieved from: https://www.ajog.org/article/S0002-9378(15)00208-2/fulltext
[22] FDA Announces New Qualified Health Claims for EPA
and DHA Omega-3 Consumption and the Risk of Hypertension and Coronary Heart Disease. FDA. 06/19/2019. Retrieved from: https://www.fda.gov/food/cfsan-constituent-updates/fda-announces-new-qualified-health-claims-epa-and-dha-omega-3-consumption-and-risk-hypertension-and
[23] Krupa K, Fritz K, Parmar M. Omega-3 Fatty Acids. National Library of Medicine. National Center for Biotechnology Information. StatPearls. Last Updated: September 26, 2022. Retrieved from: https://www.ncbi.nlm.nih.gov/books/NBK564314/ . http://creativecommons.org/licenses/by/4.0/
[24] LOVAZA- omega-3-acid ethyl esters capsule, liquid filled. Daily Med, NIH. Updated February 24, 2021. Retrieved from: https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=c1920576-1b04-4b20-bb00-061f09032574#LINK_c7c5c809-977a-411d-8b59-8bb779c73288
[25] OMTRYG- omega-3-acid ethyl esters capsule. Daily Med, NIH. Updated March 31, 2016. Retrieved from: https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=5fe15bdb-f59f-4b87-8e5d-8a3d5683eb3d
[26] SECTION ON BREASTFEEDING, Arthur I. Eidelman, Richard J. Schanler, Margreete Johnston, Susan Landers, Larry Noble, Kinga Szucs, Laura Viehmann; Breastfeeding and the Use of Human Milk. Pediatrics March 2012; 129 (3): e827–e841. Retrieved from: https://publications.aap.org/pediatrics/article/129/3/e827/31785/Breastfeeding-and-the-Use-of-Human-Milk?autologincheck=redirected?nfToken=00000000-0000-0000-0000-000000000000
[27] Dietary Guidelines for Americans 2020 – 2025. USDA. December 2020.
[28] Institute of Medicine. Dietary Reference Intakes for Energy, Carbohydrate, Fiber, Fat, Fatty Acids, Cholesterol, Protein, and Amino Acids. Washington, D. C.: National Academies Press; 2002. Retrieved from: https://nap.nationalacademies.org/read/10490/chapter/10#463
[29] Balić A et al. Omega-3 Versus Omega-6 Polyunsaturated Fatty Acids in the Prevention and Treatment of Inflammatory Skin Diseases. Int J Mol Sci. 2020;21(3):741. Published 2020 Jan 23. Retrieved from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7037798/
[30] Omega-3 and Omega-6 Content of Commonly Eaten Foods. Algae.com. Retrieved from: https://blog.algaecal.com/wp-content/uploads/PDFCommonOmega3Foods.pdf
[31] Caravita MA et al. Omega-3 / omega-6 fatty acids ratio in olive oils from Italian olive varieties. Agro Food Industry Hi Tech18(6):17-18. November 2007.
[32] Hernández ML, Sicardo MD, Belaj A, Martínez-Rivas JM. The Oleic/Linoleic Acid Ratio in Olive (Olea europaea L.) Fruit Mesocarp Is Mainly Controlled by OeFAD2-2 and OeFAD2-5 Genes Together With the Different Specificity of Extraplastidial Acyltransferase Enzymes. Front Plant Sci. 2021;12:653997. Published 2021 Mar 8. Retrieved from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7982730/
[33] Kafkaletou M, Ouzounidou G, Tsantili E. Fruit Ripening, Antioxidants and Oil Composition in Koroneiki Olives (Olea europea L.) at Different Maturity Indices. Agronomy. 2021; 11(1):122. Retrieved from: https://www.mdpi.com/2073-4395/11/1/122/htm